New England – Smocking and Mortality – Beyond Established Causes
Smoking and Mortality — Beyond Established Causes
Brian D. Carter, M.P.H., Christian C. Abnet, Ph.D., Diane Feskanich, Sc.D., Neal D. Freedman, Ph.D., Patricia Hartge, Sc.D., Cora E. Lewis, M.D., Judith K. Ockene, Ph.D., Ross L. Prentice, Ph.D., Frank E. Speizer, M.D., Michael J. Thun, M.D., and Eric J. Jacobs, Ph.D.
Etude publiée le 12 février 2015 dans la revue « New England, Journal of Medicine »
The 2014 Surgeon General’s report estimates that cigarette smoking causes more than 480,000 deaths each year in the United States.1 This widely cited estimate of the mortality burden of smoking may be an underestimate, because it considers deaths only from the 21 diseases that have been formally established as caused by smoking (12 types of cancer, 6 categories of cardiovascular disease, diabetes, chronic obstructive pulmonary disease [COPD], and pneumonia including influenza). Associations between smoking and the 30 most common causes of death in the United Kingdom in the Million Women Study suggest that the excess mortality observed among current smokers cannot be fully explained by these 21 diseases.2
We previously reported the risks associated with smoking with respect to overall mortality and five major causes of death (lung cancer, COPD, ischemic heart disease, other heart disease, and total [ischemic and hemorrhagic] stroke) in two early American Cancer Society cohorts, as well as in a contemporary population pooled from five large U.S. cohorts.3 We documented the ways in which the smoking-related risk of death from these causes has changed over the past 50 years, but we did not examine mortality from other causes. A full accounting of the mortality burden from smoking in contemporary populations requires a comprehensive examination of the causes of death.
In the current analysis, we used the same pooled contemporary cohort population3 but included 52 cause-of-death categories. Additional follow-up information and updated data on the number of deaths have been provided for some cohorts. This pooled cohort is large, which allows us to characterize associations of smoking with deaths from the entire spectrum of disease, including diseases that are relatively uncommon.
METHODS
Study Population
Study participants, 55 years of age or older, were drawn from five large U.S. cohorts for which information on smoking was obtained at least once during the follow-up period (2000 to 2011). These included the Cancer Prevention Study II Nutrition Cohort,4 the Nurses’ Health Study I cohort,5 the Health Professionals Follow-up Study cohort,6 the Women’s Health Initiative cohort,7and the National Institutes of Health–AARP Diet and Health Study cohort.8 Details of the enrollment, follow-up, and smoking assessments for each cohort are described in Section S1 in theSupplementary Appendix, available with the full text of this article at NEJM.org. Participants were excluded if their baseline smoking status was unknown (14,457 men and 11,951 women) or if their follow-up ended before January 1, 2000 (38,809 men and 58,126 women). We did not exclude participants with preexisting diseases because we wanted this analysis to be consistent with the previous report and because development of disease often lies on the causal pathway between smoking and mortality. The final pooled cohort included 421,378 men and 532,651 women.
Smoking Variables
All smoking data were self-reported. The assessments of smoking status, number of cigarettes per day, and years since cessation are described in Section 1 in the Supplementary Appendix. The responses in serial follow-up questionnaires were used to model smoking as a time-dependent variable. In the case of former smokers and persons who had never smoked, those who did not complete follow-up questionnaires retained their smoking status, and the data were not censored. In the case of current smokers, we censored data on the date of the second missed questionnaire to avoid misclassifying those who may have quit smoking.
Mortality Follow-up
Details of the mortality follow-up protocol for each cohort are available in Section 1 in theSupplementary Appendix. The Surgeon General finds the evidence sufficient to include 21 disease categories in the formal list of diseases caused by smoking.1 We examined each of these individually except for cervical cancer, which occurred only rarely in this cohort. Additional causes of death were categorized into 10 broad coding groups in the International Classification of Diseases, 10th Revision (ICD-10). We examined any specific outcome that accounted for at least 20 deaths among current smokers of either sex. Outcomes accounting for fewer deaths were aggregated within each broad ICD-10 grouping. The final analysis included 52 outcomes, including death from any cause, death from all known causes, and death from all unknown causes combined. The number of deaths in each cohort is shown in Table S1 in the Supplementary Appendix.
Statistical Analysis
The baseline date for all participants was January 1, 2000; each participant contributed person-time until the date of death, until the date on which the data were censored, or until December 31, 2011, whichever was earliest. Deaths and person-years were tabulated according to smoking status and 10-year attained-age groups, and overall mortality was standardized to the age distribution in the U.S. population in 2000. We calculated the proportional contribution of each disease to the total excess risk of death among current smokers as compared with persons who never smoked. We used Cox proportional-hazards regression with adjustment for age and cohort to estimate pooled relative risks among current and former smokers as compared with those who never smoked, using the stratified Cox procedure and further adjusting for race, educational level, and daily alcohol consumption by including variables for these factors in the model. For secondary analyses, we used Cox models with time-dependent variables for number of cigarettes per day among current smokers and number of years since cessation among former smokers. We calculated P values for trend by modeling a continuous variable for number of cigarettes per day (among only current smokers) and number of years since cessation (among only former smokers).
RESULTS
Study Population
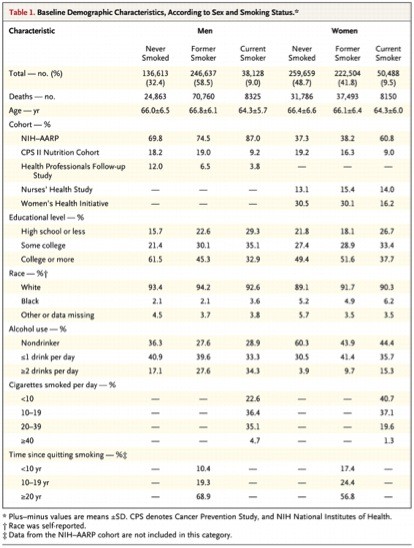
Most of the participants in the study cohorts were non-Hispanic whites and had a higher educational level than the overall U.S. population (Table 1TABLE 1Baseline Demographic Characteristics, According to Sex and Smoking Status.).9,10 Current smokers had, on average, a lower educational level than former smokers or those who had never smoked, although this difference was less pronounced among women than among men. Most former smokers reported having quit more than 10 years before the baseline date.
Smoking-Related Diseases and Mortality
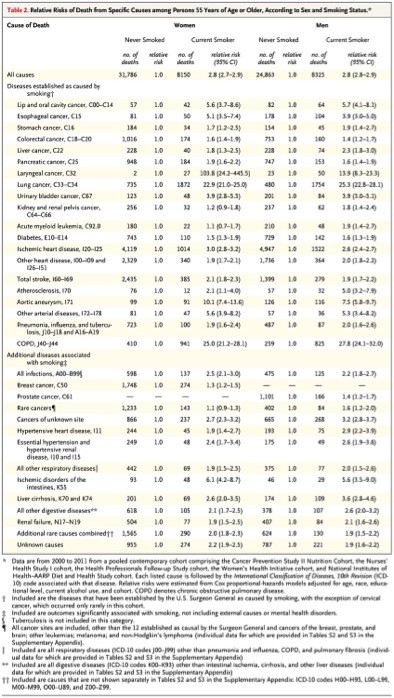
Smokers had a higher risk of death from each of the causes established as attributed to smoking than did persons who had never smoked (Table 2TABLE 2Relative Risks of Death from Specific Causes among Persons 55 Years of Age or Older, According to Sex and Smoking Status.). In analyses of diseases that are not currently established as caused by smoking, male smokers were at higher risk for death from prostate cancer (relative risk, 1.4; 95% confidence interval [CI], 1.2 to 1.7), and female smokers were at higher risk for death from breast cancer (relative risk, 1.3; 95% CI, 1.2 to 1.5). Relative risks for other causes associated with smoking were similar among men and women (Table 2); therefore, the estimates below and in Tables S4 and S5 in the Supplementary Appendix are provided for men and women combined. Current smoking was associated with a higher risk of death from infections (relative risk, 2.3; 95% CI, 2.0 to 2.7), intestinal ischemia (relative risk, 6.0; 95% CI, 4.5 to 8.1), hypertensive heart disease (relative risk, 2.4; 95% CI, 1.9 to 3.0), renal failure (relative risk, 2.0; 95% CI, 1.7 to 2.3), other respiratory diseases (relative risk, 1.9; 95% CI, 1.6 to 2.3), and liver cirrhosis (relative risk, 3.1; 95% CI, 2.6 to 3.7). Among current smokers, risks increased as the number of cigarettes smoked daily increased in the case of deaths from infections (P=0.01), breast cancer (P=0.01), and renal failure (P=0.03) (Table S4 in the Supplementary Appendix). Among former smokers, the relative risks for each of these diseases, except liver cirrhosis, declined as the number of years since quitting increased (Table S5 in the Supplementary Appendix).
Although all models were adjusted for current alcohol consumption, further analyses were restricted to persons who were not current drinkers in order to minimize potential residual confounding by alcohol use. The relative risk of death from liver cirrhosis (among men and women combined) was lower among current smokers who did not drink (relative risk, 2.0; 95% CI, 1.4 to 2.9) than it was in the overall study population, whereas the relative risk for death from breast cancer (relative risk, 1.4; 95% CI, 1.2 to 1.7) was essentially unchanged.
Current smoking was associated with higher mortality with respect to several outcomes that included multiple diseases too uncommon to examine individually. In analyses of data from men and women combined, current smoking was associated with an increased risk of death from all rare cancers combined (relative risk, 1.2; 95% CI, 1.1 to 1.4), respiratory diseases that are not included in the Surgeon General’s list (relative risk, 1.9; 95% CI, 1.6 to 2.3), rare digestive diseases that were not examined individually (relative risk, 2.2; 95% CI, 1.9 to 2.6), and all other known causes (relative risk, 2.0; 95% CI, 1.8 to 2.2).
Excess Mortality among Current Smokers
Diseases that have been established as caused by smoking accounted for approximately 83% of the total excess mortality observed among current smokers (Table 3TABLE 3Mortality and Excess Mortality, According to Sex and Smoking Status.). Most of the remaining excess mortality (16.9% among women and 15.3% among men) was accounted for by the additional outcomes shown in Table 3 and discussed above (which were selected on the basis of plausibility, incidence, and statistical significance). A small proportion was due to other, less plausibly causal, associations with outcomes, such as suicide and accidents. Relative risks for all outcomes are shown in Tables S2 and S3 in theSupplementary Appendix.
DISCUSSION
Our study provides a comprehensive, prospective analysis of the contemporary risks of death associated with cigarette smoking in the United States. The rate of death from any cause was 2 to 3 times as high among current smokers as among persons who never smoked, a finding that is consistent with the results in our previous report.3 Approximately 17% of this excess mortality was due to associations with causes that have not been formally established as attributable to smoking.
The rate of death from renal failure was twice as high among current smokers as among persons who never smoked, a finding that is consistent with results from case–control studies.11,12 Smoking is an important cause of the cardiovascular risk factors for renal failure but may also directly impair kidney function.12 Even in patients without underlying renal or cardiovascular diseases, urinary albumin, a marker of potential renal damage, increases in a dose-dependent manner with the number of cigarettes smoked per day.13
Current smoking was associated with an increased risk of death from hypertensive heart disease (according to ICD-10 coding), which is the only category of heart disease not already formally established as attributable to smoking.1 Criteria for attributing a death from heart disease to hypertensive heart disease are not well defined.14 Hypertensive heart disease can include both hypertensive heart failure and other types of heart disease. However, this association is relevant for assessing the public health burden of smoking, since a considerable number of deaths in the United States are attributed to hypertensive heart disease.15
Mortality from intestinal ischemia was strongly associated with current smoking in this cohort, as it was in the Million Women Study.2 The relative risk was approximately 6 among current smokers and decreased with increasing number of years since quitting. To our knowledge, no other large studies have examined this association. Smoking acutely reduces blood flow to the intestines,16 and evidence suggests that smoking causes risk factors that can often lead to intestinal ischemia, including atherosclerosis, platelet aggregation, and congestive heart failure.17
Mortality from infections was more than twice as high among current smokers as among persons who never smoked, and the risk increased with smoking intensity and declined with increasing number of years since cessation. Previous studies have documented higher rates of many infectious diseases among smokers.18,19 The Surgeon General has concluded that cigarette smoke adversely affects immune function and may accelerate the progression of many infectious diseases.1
Current smoking was associated with more than double the risk of death from diseases included in the category of other digestive diseases (ICD-10 codes K00–K54, K56–K69, and K78–K93). The Surgeon General recently concluded that the evidence linking smoking to Crohn’s disease was suggestive but still insufficient.1 Moreover, smoking is an important modifiable risk factor for peptic ulcers20,21 and acute pancreatitis.22,23 Other diseases in this group include paralytic ileus and bowel obstructions, cholelithiasis, diverticulitis, and gastrointestinal hemorrhages. Although these diseases are not common causes of death, they account for millions of hospitalizations each year.24
There is broad agreement that cigarette smoking causes cancers at a minimum of 12 different sites.25,26 This study updates the relative risks of death from cancer at these sites in a contemporary population. We also found additional significant associations with death from breast cancer and from prostate cancer. The Surgeon General has not yet concluded that smoking causes breast cancer.1 We found that the risk of death increased significantly with smoking intensity and declined after cessation of smoking, findings that were similar to results from previous analyses of data from the individual cohorts that were pooled for the current analysis.27-30 Numerous studies have examined the relationship between smoking and breast cancer; however, confounding by alcohol use remains a concern. An analysis of the Million Women Study showed a 13% higher risk of fatal breast cancer among current smokers after adjustment for the number of drinks per week, but no association was observed among women who consumed fewer than three drinks per week.2In our analysis, smoking remained significantly associated with death from breast cancer among women who were not current drinkers. However, associations between smoking and death from breast cancer may also be biased by differences in screening31 or treatment32 patterns among smokers, and information on these variables was not available in this study. Additional studies with detailed information on these factors may be useful in clarifying whether smoking is causally associated with death from breast cancer.
Mortality from prostate cancer in this population was 43% higher among current smokers than among those who had never smoked, a finding that is consistent with most previous analyses of prostate-cancer mortality.33 The Surgeon General concluded that although there was insufficient evidence that smoking increases the incidence of prostate cancer, the available evidence suggested that current or recent smoking increases the risk of advanced-stage disease and of death from prostate cancer.1 Higher mortality from prostate cancer among smokers could be caused by delayed diagnosis owing to less intense medical surveillance or by a promoting effect of smoking on later stages of carcinogenesis and progression.34 This latter hypothesis is supported by analyses showing associations between smoking and both progression of prostate cancer35 and prostate-cancer–specific mortality among men with prostate cancer.36 Results from our analysis appear to be consistent with an influence of smoking on later stages of carcinogenesis, since we observed no increase in prostate-cancer mortality among men who had recently quit smoking.
We found significantly higher mortality from liver cirrhosis among smokers than among persons who never smoked but did not observe a dose–response pattern with respect to smoking intensity or years since quitting. In a recent analysis of the Million Women Study, mortality from liver cirrhosis was increased by a factor of 3, a finding that was unchanged when the analysis was restricted to women who reported consuming fewer than three drinks per week.2 In our analysis, current smoking was significantly associated with death from liver cirrhosis even among persons who were not current drinkers, although the relative risk was lower in that subgroup than in the overall study population. This association may be confounded by past alcohol use, but it could plausibly be attributed, at least in part, to smoking. Future studies should focus on the risks associated with smoking among persons who have never drunk alcohol.
Overall, associations between smoking and death from the 14 disease categories shown in Table 3accounted for virtually all the excess mortality associated with smoking that was not already accounted for by diseases previously established as attributable to smoking. We think there is strong evidence for a causal association between smoking and at least 5 of these disease categories — infections, hypertensive heart disease, renal failure, intestinal ischemia, and other respiratory diseases. The associations with respiratory diseases and infections have strong biologic plausibility. Hypertensive heart disease, renal failure, and intestinal ischemia are related to poor vascular function, and the adverse effects of smoking on vascular function in general are well established.17
In addition to these five disease categories, smoking was associated with mortality from cancers of unknown primary site that was increased by a factor of nearly 3. No cancer that has not already been established as caused by smoking is likely to be as strongly associated with smoking as that. Therefore, the excess risk of death from these cancers is likely to have resulted from cancers already established as caused by smoking. The same holds true with respect to deaths from unknown causes. Since the great majority of deaths are from causes established as attributable to smoking, this category probably includes substantial numbers of deaths from known smoking-related diseases. Deaths from the five disease categories we consider likely to be causal combined with deaths from unknown cancers and unknown causes accounted for approximately 10% of the total excess mortality among smokers in this cohort, or about half of all the excess mortality not accounted for by diseases already established as caused by smoking.
Our results suggest that the Surgeon General’s recent estimate of smoking-attributable mortality may have been an underestimate. The Surgeon General’s estimate, which took into account only the 21 diseases formally established as caused by smoking, was that approximately 437,000 deaths among adults are caused each year by active smoking (not including secondhand smoke). However, the Surgeon General’s report presents an alternative estimate of 556,000 deaths among adults on the basis of the excess mortality from all causes. The difference between these two estimates is nearly 120,000 deaths.1 If, as suggested by the results in our cohort, at least half of this difference is due to associations of smoking with diseases that are causal but are not yet formally established as such, then at least 60,000 additional deaths each year among U.S. men and women may be caused by cigarette smoking.
The primary strength of this study is its large size, which enabled us to examine causes of death that are too rare to examine in smaller studies; nonetheless, these outcomes are responsible for a sizable number of smoking-related deaths. This analysis includes mortality data that are updated from our original report and thus provides more precise estimates of the contemporary risks of death associated with smoking.
A notable limitation of this study is that most members of the study population were white, and on average, they were better educated than the general population. Another limitation is that the associations observed in this study could be confounded by differences between smokers and nonsmokers with respect to risk factors including diet, physical activity, and access to medical care. The potential for confounding varies depending on the specific mortality outcome. However, in an earlier study of smoking and mortality, adjustment for demographic and behavioral factors had a minimal effect on risk estimates.37
In conclusion, this comprehensive examination of cause-specific mortality in a large contemporary population identified associations between smoking and increased mortality from several diseases that are not currently established as caused by smoking. Although these associations should be investigated further, our results suggest that the number of persons in the United States who die each year as a result of smoking cigarettes may be substantially greater than currently estimated.
Supported by the American Cancer Society.
Disclosure forms provided by the authors are available with the full text of this article at NEJM.org.
Dr. Lewis reports receiving grant support through her institution from Novo Nordisk. No other potential conflict of interest relevant to this article was reported.
SOURCE INFORMATION
From the Epidemiology Research Program, American Cancer Society, Atlanta (B.D.C., M.J.T., E.J.J.); the Division of Cancer Epidemiology and Genetics, National Cancer Institute, Bethesda, MD (C.C.A., N.D.F., P.H.); the Channing Division of Network Medicine, Department of Medicine, Brigham and Women’s Hospital and Harvard Medical School, Boston (D.F., F.E.S.); the Department of Medicine, Division of Preventive Medicine, University of Alabama at Birmingham, Birmingham (C.E.L.); the Department of Medicine, Division of Preventive and Behavioral Medicine, University of Massachusetts Medical School, Worcester (J.K.O.); and the Division of Public Health Sciences, Fred Hutchinson Cancer Research Center, Seattle (R.L.P.).